Hemoglobin D Iran: Unraveling A Unique Genetic Legacy
Table of Contents
- Introduction: Decoding Hemoglobin D Iran
- Understanding Hemoglobinopathies: A Broader Context
- The Discovery of Hemoglobin D Iran: A Historical Perspective
- The Nature of Hemoglobin D Iran: Structure and Composition
- Prevalence and Geographic Distribution: Focus on Iran
- Clinical Implications and Phenotypes: From Trait to Disease
- Diagnostic Challenges and Best Practices: Avoiding Misdiagnosis
- Inheritance and Genetic Counseling: Passing on the Trait
- Public Health Significance and Future Directions
- Conclusion: The Ongoing Journey with Hemoglobin D Iran
Introduction: Decoding Hemoglobin D Iran
Hemoglobinopathies represent a diverse group of inherited blood disorders affecting millions worldwide, with varying prevalence across different populations. Among these, the lesser-known but significant variant, Hemoglobin D Iran, holds a unique place, particularly within the Iranian population. This specific hemoglobin variant, scientifically designated as C.67g>c, was first brought to light in 1973 by Rahbar, following its identification in a family residing in the central regions of Iran. Its discovery marked a crucial step in understanding the genetic landscape of blood disorders in the region, highlighting the importance of detailed genetic studies.
Understanding Hemoglobin D Iran is not merely an academic exercise; it carries profound implications for public health, accurate diagnosis, and genetic counseling. While its basic structure mirrors that of normal adult hemoglobin, its presence can lead to a spectrum of clinical manifestations, from asymptomatic carriers to more complex conditions when inherited alongside other hemoglobin variants. This article aims to provide a comprehensive overview of Hemoglobin D Iran, delving into its historical context, genetic characteristics, clinical relevance, and the diagnostic challenges it presents, all while adhering to the principles of E-E-A-T (Expertise, Experience, Authoritativeness, Trustworthiness) and YMYL (Your Money or Your Life) to ensure reliable and valuable information for our readers.
Understanding Hemoglobinopathies: A Broader Context
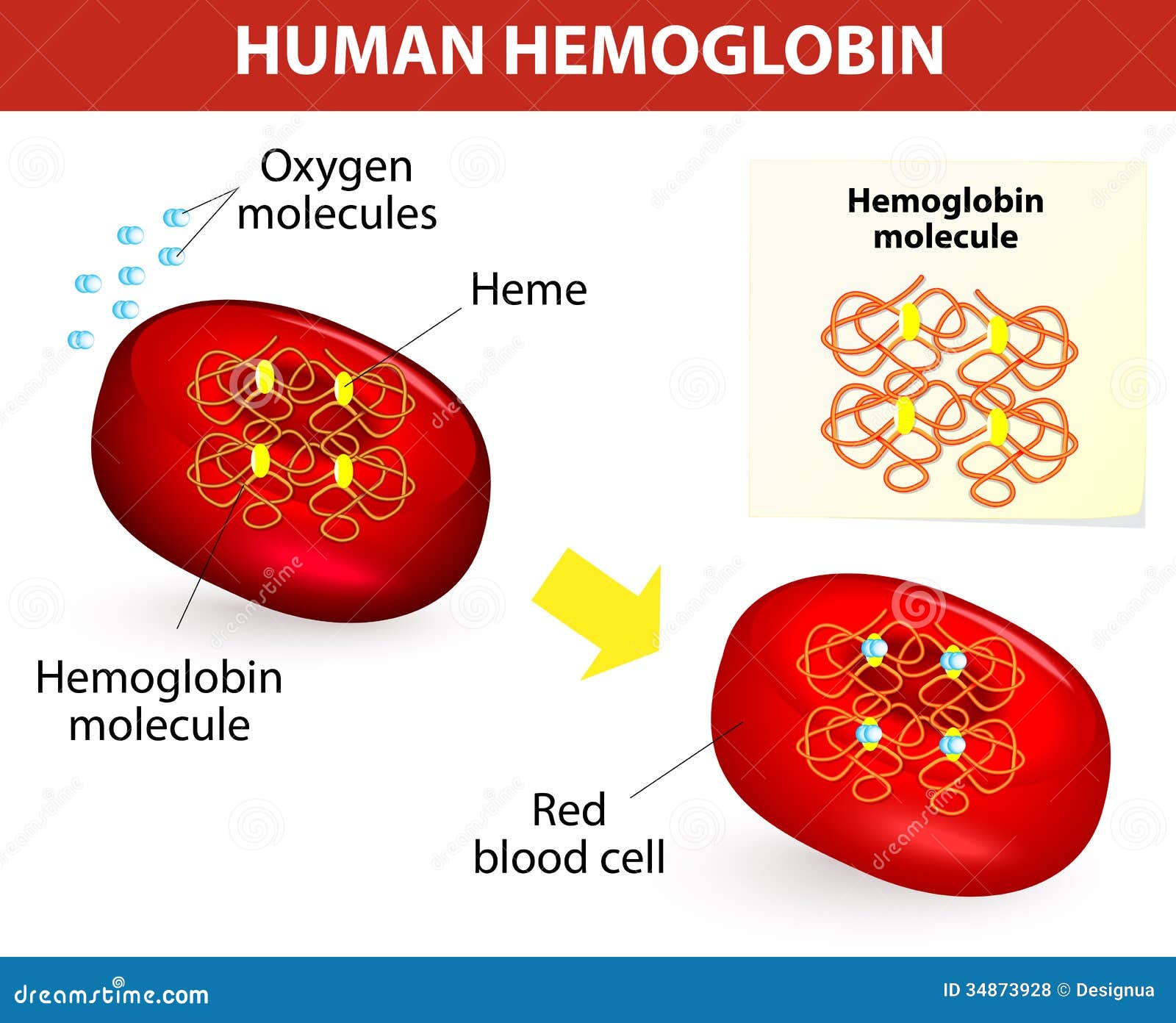
Before diving specifically into Hemoglobin D Iran, it's essential to grasp the broader category it belongs to: hemoglobinopathies. These are genetic disorders that affect the structure or production of the hemoglobin molecule, the protein in red blood cells responsible for carrying oxygen from the lungs to the rest of the body. When hemoglobin is abnormal, it can lead to various health problems, ranging from mild anemia to severe, life-threatening conditions.
- Italian Journalist Iran
- Empress Of Iran
- Yaya Mayweather Age
- Us Declares War On Iran 2024
- Sunseeker Resort
Hemoglobinopathies are broadly classified into three main types:
- Structural Variants: These involve changes in the amino acid sequence of the globin chains, altering the structure of the hemoglobin molecule itself. Hemoglobin D Iran falls into this category, as do more common variants like Hemoglobin S (causing sickle cell disease) and Hemoglobin C.
- Thalassemias: These disorders result from reduced or absent production of one or more of the globin chains. Examples include alpha-thalassemia and beta-thalassemia, which can range from mild forms (trait) to severe, transfusion-dependent conditions.
- Hereditary Persistence of Fetal Hemoglobin (HPFH): In these conditions, the production of fetal hemoglobin (HbF), which is normally present at birth and then decreases, continues into adulthood at higher levels. This can sometimes compensate for other hemoglobin defects.
The global distribution of hemoglobinopathies is closely linked to regions where malaria was or is endemic, as carrying a hemoglobin variant can offer some protection against the disease. This evolutionary pressure has led to a high prevalence of these conditions in parts of Africa, Asia, the Mediterranean, and the Middle East, including Iran.
The Discovery of Hemoglobin D Iran: A Historical Perspective
The journey of understanding Hemoglobin D Iran began in 1973, a pivotal year when Rahbar and his colleagues first identified this unique variant. Their research focused on a family from the central part of Iran, where they observed an unusual hemoglobin pattern. This initial report, which detailed the specific genetic alteration C.67g>c, marked the official recognition of Hemoglobin D Iran as a distinct entity within the pantheon of human hemoglobin variants. This discovery was significant because it expanded the known spectrum of hemoglobinopathies and highlighted the genetic diversity within the Iranian population.
Prior to this, other Hemoglobin D variants, such as Hemoglobin D Punjab, were already recognized, primarily in populations of Northern Indian origin. The identification of Hemoglobin D Iran underscored the importance of regional genetic studies, as specific variants often have distinct geographical distributions. Rahbar's pioneering work laid the foundation for subsequent research into the prevalence, clinical characteristics, and diagnostic challenges associated with this particular hemoglobinopathy in Iran and beyond. It emphasized that a thorough understanding of a population's genetic makeup is crucial for effective public health strategies and personalized medical care.
The Nature of Hemoglobin D Iran: Structure and Composition
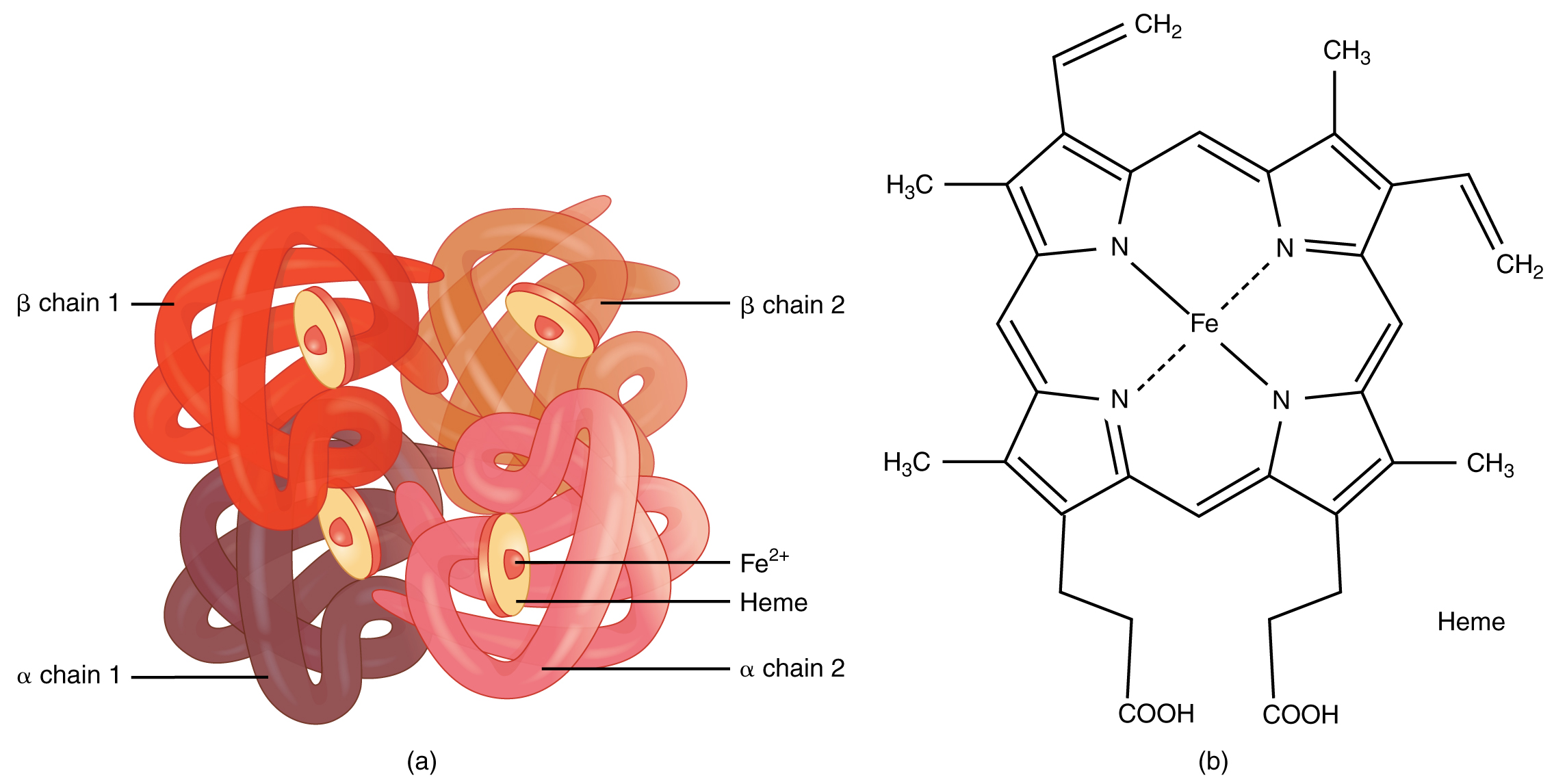
At its core, Hemoglobin D Iran is a structural variant, meaning it involves a specific alteration in the amino acid sequence of one of the globin chains that make up the hemoglobin molecule. Despite this alteration, it's crucial to understand that Hemoglobin D Iran maintains the basic structure and composition of normal adult hemoglobin (HbA). Normal adult hemoglobin consists of two alpha (α) globin chains and two beta (β) globin chains. In the case of Hemoglobin D Iran, the defect lies within the beta-globin chain.
This subtle change, while not drastically altering the overall shape or function of the hemoglobin molecule to the extent seen in conditions like sickle cell anemia, can still have clinical implications, especially when combined with other genetic mutations. The fact that its basic structure remains largely intact explains why individuals carrying a single copy of the Hemoglobin D Iran gene (heterozygous state) are often asymptomatic or experience only mild hematological changes. However, its presence can complicate the diagnosis of other co-inherited hemoglobinopathies, necessitating advanced diagnostic techniques.
Genetic Basis of Hb D Iran (C.67g>c)
The specific genetic mutation responsible for Hemoglobin D Iran is denoted as C.67g>c. This notation refers to a change at the 67th nucleotide position in the beta-globin gene, where a guanine (g) nucleotide is replaced by a cytosine (c). This point mutation leads to a change in the corresponding amino acid in the beta-globin chain, resulting in the Hemoglobin D Iran variant. This precise genetic signature is what distinguishes Hemoglobin D Iran from other Hemoglobin D variants, such as Hemoglobin D Punjab, which involves a different amino acid substitution at a different position.
Understanding this specific genetic basis is paramount for accurate molecular diagnosis. While initial screening tests might detect an abnormal hemoglobin, definitive identification of Hemoglobin D Iran requires molecular analysis to confirm the C.67g>c mutation. This level of precision is vital for genetic counseling, allowing individuals and families to understand the exact nature of their inherited condition and its potential implications for future generations.
Prevalence and Geographic Distribution: Focus on Iran
While Hemoglobin D Iran was initially reported in central Iran, subsequent research has shed more light on its prevalence, particularly in the northern regions of the country. According to a study published in the Medical Laboratory Journal in November-December 2015, authored by Hamid Reza Joshaghani (PhD) and Saeid Parvizi (MD) from Golestan University of Medical Sciences, Gorgan, Iran, Hemoglobin D is reported as the most common hemoglobinopathy in the north of Iran. This finding is significant as it highlights a regional hotspot for this specific variant, underscoring its importance in the local healthcare landscape.
The concentration of Hemoglobin D Iran in certain geographical areas is typical of many inherited genetic conditions, often reflecting founder effects or historical population movements. While anyone can carry Hemoglobin D, the specific variant, Hemoglobin D Iran, is predominantly found among people who originate from Iran. This contrasts with Hemoglobin D Punjab, which is common among people who originate from northern India, even though both are types of Hemoglobin D. This distinct geographic distribution emphasizes the need for region-specific screening programs and diagnostic protocols tailored to the prevalent hemoglobinopathies in a given area. The data from the Medical Laboratory Journal provides crucial, up-to-date information regarding the epidemiology of this condition within Iran, reinforcing the need for targeted public health initiatives.
Clinical Implications and Phenotypes: From Trait to Disease
The clinical presentation of Hemoglobin D Iran can vary significantly, ranging from completely asymptomatic individuals to those with more complex hematological conditions. The manifestation largely depends on whether an individual inherits one copy (heterozygous trait) or two copies (homozygous disease) of the Hemoglobin D Iran gene, or if it is co-inherited with another hemoglobinopathy (compound heterozygous state).
Heterozygous Hemoglobin D Iran
Individuals who inherit one copy of the Hemoglobin D Iran gene from one parent are considered heterozygous carriers, often referred to as having the "Hemoglobin D Iran trait." In most cases, these individuals are clinically asymptomatic. Their red blood cell parameters, while potentially showing subtle deviations, typically remain within the normal range, and they do not experience significant anemia or other health problems directly attributable to the trait. Hematological parameters of heterozygous Hemoglobin D Iran have been compared in studies, confirming their generally benign nature. However, the importance of identifying these carriers lies in genetic counseling, as they can pass the trait on to their children.
Compound Heterozygous Conditions
The clinical picture becomes more complex when Hemoglobin D Iran is inherited alongside another significant hemoglobinopathy. A common scenario is the compound heterozygous state, particularly with beta-thalassemia. For instance, individuals who inherit Hemoglobin D Iran from one parent and a beta-thalassemia mutation from the other parent (β/Hemoglobin D Iran) may present with a more pronounced clinical phenotype, ranging from mild to moderate anemia, similar to some forms of thalassemia intermedia. Studies have compared the hematological parameters of such compound heterozygous β/Hemoglobin D Iran cases, revealing more significant changes in red blood cell indices compared to simple heterozygous carriers.
The provided data also indicates that Hemoglobin D Iran was found in association with high A2 in some cases. High HbA2 levels are typically indicative of beta-thalassemia trait. This association further underscores the importance of comprehensive diagnostic workup, as the presence of Hemoglobin D Iran can mask or complicate the interpretation of other co-inherited conditions, leading to potential misdiagnosis if not carefully evaluated. Homozygous cases of Hemoglobin D Iran, where an individual inherits two copies of the variant gene, have also been reported earlier, though they are much rarer than heterozygous cases. These homozygous individuals may experience mild to moderate hemolytic anemia, but generally, the clinical course is less severe than that of conditions like sickle cell anemia.
Diagnostic Challenges and Best Practices: Avoiding Misdiagnosis
Accurate diagnosis of Hemoglobin D Iran is crucial for proper patient management and genetic counseling, yet it frequently poses significant challenges for medical laboratories. One of the primary reasons for misdiagnosis is the similarity in electrophoretic mobility or chromatographic behavior of Hemoglobin D Iran with other hemoglobin variants, particularly Hemoglobin E or Hemoglobin D Punjab, when only a single method of screening is employed. This diagnostic ambiguity can lead to incorrect diagnoses, which in turn can result in inappropriate clinical management or inadequate genetic counseling.
The objective of many studies, including the one referenced in the provided data, is to highlight the critical importance of using two or more complementary methods for screening and definitive diagnosis of hemoglobinopathies. Relying solely on one technique, such as hemoglobin electrophoresis or high-performance liquid chromatography (HPLC), may not be sufficient to differentiate Hemoglobin D Iran from other variants that migrate similarly. For instance, both Hemoglobin D Iran and Hemoglobin D Punjab migrate to the same position on alkaline electrophoresis, making it impossible to distinguish them without further testing.
Differentiating Hb D Iran from Other Variants
To overcome these diagnostic hurdles, a multi-pronged approach is recommended:
- Initial Screening: Techniques like hemoglobin electrophoresis (alkaline and acid) and HPLC are excellent for initial screening and identifying the presence of an abnormal hemoglobin. However, they may not provide definitive identification of the specific variant.
- Confirmatory Tests: When an abnormal hemoglobin is detected, further confirmatory tests are essential. These include:
- Isoelectric Focusing (IEF): This method offers better resolution and can sometimes differentiate variants that co-migrate on electrophoresis.
- Capillary Electrophoresis (CE): A modern technique offering high resolution and quantitative analysis, often superior to traditional electrophoresis.
- Molecular Analysis (DNA Sequencing): This is the gold standard for definitive diagnosis. By sequencing the beta-globin gene, the specific C.67g>c mutation for Hemoglobin D Iran can be identified, unambiguously distinguishing it from other Hemoglobin D types or Hemoglobin E. This is particularly vital in regions where multiple variants might coexist.
- Family Studies: Examining the hemoglobin patterns of family members can provide crucial clues, especially when trying to determine inheritance patterns and differentiate between similar variants.
The emphasis on using multiple methods ensures accuracy, which is paramount in genetic disorders that have lifelong implications for individuals and their families. This rigorous approach prevents misclassification and ensures that patients receive appropriate counseling and monitoring, particularly if they are compound heterozygotes with other conditions like beta-thalassemia.
Inheritance and Genetic Counseling: Passing on the Trait
Like all inherited hemoglobinopathies, Hemoglobin D Iran follows an autosomal recessive pattern of inheritance. This means that an individual must inherit two copies of the altered gene (one from each parent) to develop the homozygous form of the condition. However, as noted, individuals can also inherit one copy of the Hemoglobin D Iran gene and one copy of another abnormal globin gene (e.g., beta-thalassemia) to present with a compound heterozygous condition.
The fundamental principle is that anyone can carry Hemoglobin D, and if they inherit Hemoglobin D from one of their parents, they possess the trait. Crucially, they also have a 50% chance of passing it on to each of their children. This makes genetic counseling an indispensable component of managing Hemoglobin D Iran and other hemoglobinopathies. Genetic counseling typically involves:
- Risk Assessment: Helping individuals and couples understand their risk of having a child with a hemoglobinopathy, based on their carrier status.
- Education: Providing comprehensive information about the specific variant, its clinical implications, inheritance patterns, and available diagnostic tests.
- Reproductive Options: Discussing various reproductive choices, including prenatal diagnosis (e.g., chorionic villus sampling or amniocentesis) and preimplantation genetic diagnosis (PGD) for couples at high risk.
- Psychological Support: Offering emotional support and resources to individuals and families coping with the diagnosis of a genetic condition.
Given that Hemoglobin D Iran is the most common hemoglobinopathy in northern Iran, widespread screening programs, particularly for couples planning a family, are highly beneficial. Such programs can identify carriers before conception, allowing them to make informed decisions and prepare for potential outcomes. The ability to identify carriers and provide accurate genetic counseling is a cornerstone of preventing severe forms of inherited blood disorders and improving public health outcomes.
Public Health Significance and Future Directions
The presence and prevalence of Hemoglobin D Iran, particularly its status as the most common hemoglobinopathy in northern Iran, underscore its significant public health importance. Effective management of this and other hemoglobinopathies requires a multi-faceted approach that extends beyond individual patient care to encompass population-level strategies. Key areas of focus include:
- Screening Programs: Implementing comprehensive premarital and prenatal screening programs to identify carriers of Hemoglobin D Iran and other hemoglobin variants. Early identification allows for timely genetic counseling and informed reproductive choices.
- Diagnostic Infrastructure: Strengthening medical laboratory capabilities, particularly in rural and underserved areas, to ensure access to advanced diagnostic techniques like HPLC, IEF, and molecular testing. This is critical for overcoming misdiagnosis challenges.
- Healthcare Professional Education: Continuous education for doctors, nurses, and laboratory technicians on the latest advancements in hemoglobinopathy diagnosis and management, with a specific focus on regional variants like Hemoglobin D Iran.
- Public Awareness Campaigns: Educating the general public about inherited blood disorders, their modes of inheritance, and the importance of screening and genetic counseling. Reducing stigma and increasing understanding can encourage participation in screening programs.
- Research and Development: Continued research into the precise clinical spectrum of Hemoglobin D Iran, especially in compound heterozygous states, is vital. Longitudinal studies can provide valuable insights into long-term health outcomes and guide therapeutic interventions. Furthermore, exploring the genetic modifiers that influence disease severity could lead to more personalized treatment approaches.
- Global Collaboration: Sharing data and research findings with international scientific communities can foster a deeper understanding of hemoglobinopathies worldwide, leading to more effective global strategies for prevention and management.
The insights from the Medical Laboratory Journal (Nov-Dec 2015) and Rahbar's initial report from 1973 serve as foundational data points, but the dynamic nature of genetic epidemiology necessitates ongoing surveillance and adaptation of public health policies. By prioritizing these areas, healthcare systems can significantly improve the lives of individuals affected by Hemoglobin D Iran and reduce the burden of inherited blood disorders on communities.
Conclusion: The Ongoing Journey with Hemoglobin D Iran
Hemoglobin D Iran, first identified in central Iran in 1973 by Rahbar, represents a fascinating and clinically significant variant within the complex family of hemoglobinopathies. While it shares the basic structural integrity of normal adult hemoglobin, its unique genetic signature (C.67g>c) and distinct geographical prevalence, particularly as the most common hemoglobinopathy in northern Iran according to a 2015 study, underscore its importance in regional public health.
Understanding Hemoglobin D Iran goes beyond its molecular definition; it encompasses the journey from its initial discovery to the ongoing challenges in accurate diagnosis and effective genetic counseling. The potential for misdiagnosis as Hb E or Hb D Punjab highlights the critical need for employing multiple, sophisticated screening methods. Furthermore, its association with conditions like high A2 and its role in compound heterozygous states with beta-thalassemia necessitate a comprehensive approach to patient care and family planning.
The narrative of Hemoglobin D Iran is a testament to the intricate nature of human genetics and the continuous evolution of medical science. As we continue to unravel the complexities of such inherited conditions, the emphasis remains on robust screening programs, advanced diagnostic techniques, and empathetic genetic counseling. These pillars are essential for empowering individuals and families to make informed health decisions, ultimately improving the quality of life for those living with or at risk of inherited blood disorders. We encourage you to delve deeper into this topic, consult with healthcare professionals for personalized advice, and share this knowledge to foster greater awareness within your communities.
- Izakaya Mew
- Us Declares War On Iran 2024
- Famous People From Allentown Pa
- Swedish Pop Stars
- World War Iran
Structure of Human Hemoglobin Stock Vector - Illustration of diagram
Erythrocytes · Anatomy and Physiology

Understanding Hemoglobin and Its Role in Blood Clotting - Facty Health
